Long before Emery N. Brown chaired Massachusetts General Hospital (MGH)’s recent 175th anniversary celebration of the first public demonstration of ether anesthesia, he was thinking deeply about how far anesthesiology has come and could still go.
Anesthetic drugs act on the brain, but the field has barely explored the innovations that could come from integrating neuroscience into anesthesiology practice, says Brown, Edward Hood Taplin Professor of Medical Engineering and Computational Neuroscience. A neuroscientific approach could reduce side effects, make drug delivery more precise, manage post-operative pain better, and usher in new treatments for sleep or methods for coma recovery.
Brown performs neuroscience and statistical research in The Picower Institute for Learning and Memory and the Institute for Medical Engineering and Science and puts it into practice as an anesthesiologist at MGH. Now he is working on the development of a new research center. The Picower Institute recently spoke with him about these ideas.
Q: After 175 years of history, what are the frontiers for anesthesiology now?
A: The first public demonstration of ether anesthesia at MGH was really the start of a new era in medicine. It changed surgery overnight from being a trauma to being a reasonable and life-saving therapy. The focus of research at the time had been on coming up with better contraptions to hold you down so they could conduct a surgical procedure without anything to effectively mitigate the pain. In this regard, the field has come quite a long distance.
On the other hand, the neuroscience of anesthesia has been slow to be developed. That's what we've been working on over the last several years, and I think that's where I see the future being. The frontier in anesthesiology lies in neuroscience.
Q: What has your recent research shown about the neuroscience of anesthesia?
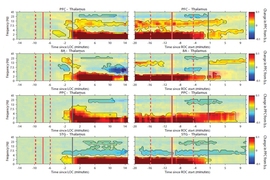
A: We now have a lot of detailed, hard data showing that anesthetic drugs create oscillations in brain circuits that impede the ability of various parts of the brain to communicate.
In recent work with my colleague Earl Miller, we came to appreciate how far away the dynamics of brain oscillations under anesthesia are from the dynamics the animals showed when conscious. You dramatically alter how much the neurons spike. What propofol is doing is slowing down brain oscillations to create an alternate dynamic, one which doesn't allow you to be conscious. The same thing is true with ketamine, but instead of the brain being slowed down, slow activity oscillates with faster activity at a very regular pace. This is also a dynamic that is quite far from the dynamic we see when an animal is conscious.
So becoming unconscious with anesthetics is not so much about turning the brain “off” as changing the dynamics. We see this in humans, too, and that's extremely helpful to us, because now I can interpret the oscillations I see when a patient is anesthetized in the operating room. I have very good neurophysiological evidence as to why I should feel comfortable the person is unconscious in those conditions. We can measure these oscillations in real time via EEG. I do it with all my patients. I'm encouraging colleagues to do it as well.
Q: What advances do you hope will arise from the new research center you are working to develop?
A: I couldn't be more excited about setting up the center because neuroscientific ideas can be turned into new approaches to taking care of patients.
For example, those oscillations that are part of the mechanism through which anesthetics induce unconsciousness are also part of the mechanism through which the drugs contribute to brain dysfunction after surgery, which we know is highly prevalent in older patients. What we have to do is develop alternate ways to inactivate circuits, so that we can create the states and do away with the side effects.
We need to take on anesthesia as a neuroscience question to address how we can develop very precise ways to control the delivery of anesthesia so the person gets just enough — not too much or not too little. How can we develop procedures to accurately read and interpret the EEG during surgery, so the anesthesiologist can reliably know when a patient is unconscious? How can we develop accurate ways of measuring the level of nociception, meaning pain that a patient is perceiving during surgery, so we can more accurately titrate analgesics during surgery? How do we work out ways to turn brain communication back on so that we can restore functionality once someone’s anesthesia is completed?
A long-range goal will be to have very site-specific methods to activate or inactivate only the brain regions and circuits that are necessary and leave the other areas untouched.
To do this we need deep neuroscience and engineering expertise. What better place than MIT, in collaboration with our clinical colleagues at MGH? It’s the perfect marriage, if you will.
There's even greater potential as we learn fundamental things about the brain from studying how anesthesia affects inter-regional communication and inhibitory networks. We can develop better ways to control the “on” and “off” of brain communication. Maybe that's a new approach for helping someone sleep better, or if we're able to reboot the brain from a very fundamental level, maybe that's a way to help foster coma recovery.