Drugs that block enzymes called tyrosine kinases are among the most effective targeted therapies for cancer. However, they typically work for only 40 to 80 percent of the patients who would be expected to respond to them.
In a new study, MIT researchers have figured out why those drugs don’t work in all cases: Many of these tumors have turned on a backup survival pathway that helps them keep growing when the targeted pathway is knocked out.
“This seems to be hardwired into the cells and seems to be providing activation of a critical survival pathway in cancer cells,” says Forest White, the Ned C. and Janet C. Rice Professor of Biological Engineering at MIT. “This pathway allows the cells to be resistant to a wide variety of therapies, including chemotherapies.”
Additionally, the researchers found that they could kill those drug-resistant cancer cells by treating with both a tyrosine kinase inhibitor and a drug that targets the backup pathway. Clinical trials are now underway to test one such combination in lung cancer patients.
White is the senior author of the study, which appears this week in the Proceedings of the National Academy of Sciences. Cameron Flower PhD ’24, who is now a postdoc at Dana-Farber Cancer Institute and Boston Children’s Hospital, is the paper’s lead author.
Tumor survival
Tyrosine kinases are involved in many signaling pathways that allow cells to receive input from the external environment and convert it into a response such as growing or dividing. There are about 90 types of these kinases in human cells, and many of them are overactive in cancer cells.
“These kinases are very important for regulating cell growth and mitosis, and pushing the cell from a nondividing state to a dividing state depends on the activity of a lot of different tyrosine kinases,” Flower says. “We see a lot of mutations and overexpression of these kinases in cancer cells.”
These cancer-associated kinases include EGFR and BCR-ABL. Many cancer drugs targeting these kinases, including imatinib (Gleevec), have been approved to treat leukemia and other cancers. However, these drugs are not effective for all of the patients whose tumors overexpress tyrosine kinases — a phenomenon that has puzzled cancer researchers.
That lower-than-expected success rate motivated the MIT team to look into these drugs and try to figure out why some tumors do not respond to them.
For this study, the researchers examined six different cancer cell lines, which originally came from lung cancer patients. They chose two cell lines with EGFR mutations, two with mutations in a tyrosine kinase called MET and two with mutations in a tyrosine kinase called ALK. Each pair included one line that responded well to the tyrosine kinase inhibitor targeting the overactive pathway and one line that did not.
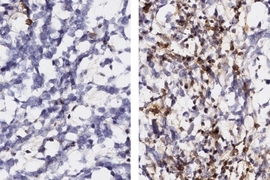
Using a technique called phosphoproteomics, the researchers were able to analyze the signaling pathways that were active in each of the cells, before and after treatment. Phosphoproteomics is used to identify proteins that have had a phosphate group added to them by a kinase. This process, known as phosphorylation, can activate or deactivate the target protein.
The researchers’ analysis revealed that the drugs were working as intended in all of the cancer cells. Even in resistant cells, the drugs did knock out signaling by their target kinase. However, in the cells that were resistant, an alternative network was already turned on, which helped the cells survive in spite of the treatment.
“Even before the therapy begins, the cells are in a state that intrinsically is resistant to the drug,” Flower says.
This survival network consists of signaling pathways that are regulated by another type of kinases known as SRC family kinases. Activation of this network appears to help cancer cells proliferate and possibly to migrate to new locations in the body. In addition to lung cancer, researchers from White’s lab have also found SRC family kinases activated in melanoma cells, where they also play a role in drug resistance, and in glioblastoma, a type of brain cancer.
“As inhibitors for SRC kinases are also drugs, the work suggests that combining inhibitors of driver oncogenes with SRC inhibitors could increase the number of patients who would benefit. This strategy merits testing in new clinical trials,” says Benjamin Neel, a professor of medicine at NYU Grossman School of Medicine, who was not involved in the study.
These findings might also explain why some patients who initially respond to tyrosine kinase inhibitors end up having their tumors recur later; the cells may end up activating this same survival pathway, but not until sometime after the initial treatment.
Combating resistance
The researchers also found that treating the resistant cells with both a tyrosine kinase inhibitor and a drug that inhibits SRC family kinases led to much greater cell death rates. By coincidence, a clinical trial testing the combination of a tyrosine kinase inhibitor called osmertinib and an SRC inhibitor is now underway, in patients with lung cancer. The MIT team now hopes to work with the same drug company to run a similar trial in pancreatic cancer patients.
The researchers also showed that they could use phosphoproteomics to analyze patient biopsy samples to see which cells already have the SRC pathways turned on.
“We are really excited to watch these clinical trials and to see how well patients do on these combinations. And I really think there’s a future for using tyrosine phosphoproteomics to guide this clinical decision-making,” White says.
This therapy might also be useful for patients whose tumors are originally susceptible to tyrosine kinase inhibitors but then later become resistant by turning on SRC pathways.
“Among the sensitive cells, some of them are able to upregulate this survival pathway and survive, which might be the residual disease that’s still there after treatment,” White says. “One of the interesting avenues here is, could we improve therapy for almost everybody, regardless of whether their tumors have intrinsic or adaptive resistance?”
The research was funded by the National Institutes of Health and the MIT Center for Precision Cancer Medicine.